38 Year old male with Fever Since 4 days
This is an online E-log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient centered online learning portfolio and your valuable comments on comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
Chief complaints-
36 yr old male patient presented to opd with
c/o Fever since 4 days
C/o of 7 episodes of loose stools
HOPI-
Patient was apparently asymptomatic 4 days back then developed fever associated with chills and rigor , No diurnal variation,relieved with medication
C/O Loose stools since yesterday,4-6 episodes/day,non blood stained
H/O anorexia present since 4 days
No H/O vomitings, decreased Urine output
No complaints of PainAbdomen/Or any bleeding manifestations
i.e., Nohematuria/ Melena or blood
in stool/Bleeding gums
Petechiae /rash.
No SOB/chest pain/palpitations
PAST HISTORY-
Not a k/c/o HTN, DM, CVA, CAD, TB, Asthma, or thyroid disorders.
Allergic history:-
No history of any kind of allergies to food/drugs
Family history:-
No significant family history
GENERAL EXAMINATION:-
THE PATIENT IS CONSCIOUS COHERENT AND COOPERATIVE
NO PALLOR ; ICTERUS; CLUBBING; CYANOSIS; ODEMA ; LYMPHADENOPATHY
TEMPERATURE:- 98.8 F
PR:81bpm
BP:110/70 mmHg
RR:17cpm


SYSTEMATIC EXAMINATIONS:-
CVS:S1 S2+,NO MURMURS
CNS: NAD
RS:BAE+ ; NVBS
P/A:SOFT ; NON TENDER ; NO ORGANOMEGALY
PROVISIONAL DIAGNOSIS:-
? Viral hemorrhagic fever
? Dengue
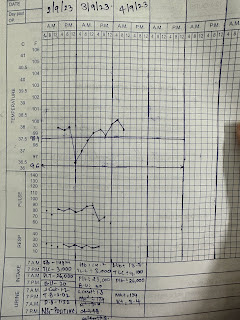
2/9/23-
HAEMOGLOBIN
14
TOTAL COUNT
3,000
NEUTROPHILS
48
LYMPHOCYTES
41
EOSINOPHILS
00
MONOCYTES
10
BASOPHILS
01
PCV
43.8
MCV
81.2
MCH
31.3
MCHC
38.6
RDW-CV
12.7
RDW-SD
35.3
RBC COUNT
5.35
PLATELET COUNT 27000
Total Bilirubin 2.04
Direct Bilirubin 1.22
SGOT(AST) 36
SGPT(ALT) 197
ALKALINE PHOSPHATE 267
UREA 30
CREATININE 1.2
UC 2.3
Sodium - 136
Potassium- 3.5
Chloride - 96
NS1 - POSITIVE
Ig M - negative
Ig G - negative
3/9/23
Hb-14.2
Total count-3000
Plt count- 23000
Blood urea- 30
S.creat- 1.3
S.Na+-131
S.K+ 3.4
S.chloride- 98
SDP transfusion done on 3/8/23 6 pm
4/8/23
Hb- 13.7
Total count- 4,100
Neutrohil-50
Lymphocytes-38
Eosinophils- 02
Monocytes-10
Basophils- 00
Pcv- 36
Mcv- 82
Platelet count-26000
Treatment-
1.I.v fluids 2 N.S @100 ml/hr
2.Tab.Dolo 650 mg Po/SOS
3.Inj. Neomol 1 gm Iv/ SOS
4.Tab.sporolac Ds Po/TID
5.Tab. Redotril 100 mg Po/OD
6.Watch for bleeding manisfestations.



Comments
Post a Comment